
(Credit-Canva)
Wildfire Smokes Are Not Just Bad For Your Respiratory Health, But Also Your Mental Health
When news of wildfires spreads, the first things people worry about is how it will affect their health. Your respiratory health may take a hit, but so will your mental health. A new study published in JAMA Network Open April 2025 has brought up the chances of increased mental health issues from wildfire smoke.
This study found that our lungs are not the only ones that are affected by the smoke, our mind is also in the mix. The wildfire smoke had an unexpected effect on people. The research found a clear connection between smoke and people who have depression, anxiety or mood swings. This means that when there are wildfires, we need to think not only about the physical dangers but also about how the smoke can impact how people feel and think.
Why Does Smoke Affect Our Mental Health?
The study explains that wildfire smoke does more than just make it hard to breathe. The research suggests that the smoke itself might directly make mental health conditions like feeling down, worried, or having mood swings worse. It's not just the stress of the fire itself that causes these problems; there might be something in the smoke that affects our brains and emotions. This is an important finding because it means we need to understand all the ways that wildfire smoke can harm our health, including our mental health.
The study mentioned PM2.5 matter which is a mixture of solid and liquid particles suspended in the air and is explicitly mentioned as a key component of wildfire smoke pollution. A study published in BMC Public Health 2022 notes that there are many physical health harms of PM2.5 and suggests a growing recognition of its link to mental well-being.
To figure this out, the scientists looked closely at the number of tiny bits of pollution in the air caused by wildfires in California during a really bad fire season in 2020. This was when there were a lot of big fires that lasted for a long time. The researchers then took this information about how much smoke was in the air each day and compared it to how many people went to the emergency room for mental health problems on those same days. By looking at these two sets of information together, they could see if there was a link between bad smoke days and more mental health emergencies.
Rise In Mental Health Emergencies
Researchers found that when the smoke from wildfires was really bad, more people went to the hospital emergency room because of mental health issues. On days with the most smoke in the air, there was a noticeable increase in the number of people needing urgent help for things like anxiety, depression, and other mood problems. This shows that the poor air quality caused by wildfire smoke can be a trigger for serious mental health difficulties, making people feel so unwell that they need to seek immediate medical attention. It highlights the immediate impact that wildfire smoke can have on mental well-being.
Even a small increase in the amount of wildfire smoke particles in the air made it more likely for people to have mental health issues that were serious enough to go to the ER. For every tiny bit more smoke in the air, they saw a small but significant rise in the number of people seeking help for things like general mental health problems, like depression, mood disorders, and anxiety. This helps us understand just how much even a little bit of wildfire smoke can affect our mental well-being.
Some groups of people were more likely to have mental health problems because of the wildfire smoke. Women had a higher chance than men, and children were even more affected. As wildfires become more common and worse because of climate change, making sure everyone has fair access to the support they need is crucial.

Credits: UNICEF
Polio Cases On The Rise Again, WHO Warns The World To A Growing Threat
The international public health community was hopeful that polio—the crippling viral illness that previously paralyzed hundreds of thousands of children every year—was almost extinct. But in a concerning twist in 2025, the World Health Organization (WHO) has raised the alarm- polio is back, and eradication hangs in the balance.
In 2020, the world celebrated a milestone—polio was officially eradicated everywhere except two nations. But in the first quarter of 2025, an old nemesis has reappeared. Cases of wild poliovirus are again increasing in Pakistan and Afghanistan, the final two bastions of endemic transmission. Pakistan, which had reported 74 cases in 2024, has already seen 6 new cases this year. Afghanistan is not far behind with 1 reported case.
While the numbers are small in themselves, they portend a worrisome trend in a decades-long fight. Global health professionals point to interruptions of vaccine campaigns—interruptions they say are directly caused by deep reductions in international assistance.
One major factor behind this upsurge is the abrupt interruption of funding support from the United States Agency for International Development (USAID). USAID has long been a pillar of support for vaccination activities in polio-endemic and high-risk areas by financing personnel, logistics, vaccine sourcing, and outreach.
A private memo by Nicholas Enrich, USAID acting assistant administrator for global health, cautions that if these pauses in funding continue, we will witness another 200,000 cases of polio paralysis each year, and hundreds of millions more are at risk of being infected. The International Rescue Committee (IRC), which was carrying out polio vaccinations under the watch of the Ministry of Health and World Vision in Kenya, says its USAID-funded program was the initial one to close on January 31st.
"Right now, IRC support for polio immunization in Kenya's hard-to-reach areas has come to a halt," confirms Mohamed El Montassir Hussein, Kenya's IRC country director. Although local health officials are still immunizing, their efforts are strained without foreign funding.
Why Does Wild Polio Persist in Just Two Countries?
Pakistan and Afghanistan are the exceptions to an otherwise polio-free world. Several chronic challenges, according to experts, include unstable security environments, misinformation, religious and political opposition to vaccination, and weak health infrastructures. Additionally, vaccination teams working in war zones frequently encounter logistical challenges and safety threats.
The virus has been extremely resilient. It takes advantage of holes in immunity caused by lack of vaccinations. Adding to the problem is the presence of circulating vaccine-derived poliovirus (cVDPV)—an uncommon event whereby the attenuated virus contained within oral polio vaccines changes and becomes virulent again.
WHO Flags High-Risk Nations and Rising Global Concern
The WHO has listed five countries with the immediate risk of the international spread of polio:
- Afghanistan
- Pakistan
- Mozambique
- Democratic Republic of Congo
- Guinea
Furthermore, 35 nations have recorded imported cases of cVDPV type 2, while 10 countries continue to experience active circulation of wild-type or vaccine-derived poliovirus in the last 24 months. WHO's guidelines are:
- Improved vaccine coverage
- Increased access to healthcare in risk areas
- Travel restrictions for unvaccinated travelers from high-risk areas
But with more than $200 million in donor funding lost— including life-saving funds from the U.S. President's Emergency Plan for AIDS Relief (PEPFAR)—these guidelines encounter tremendous implementation challenges.
Hidden Cost of Underfunding Global Health
It is the invisible spread that makes the situation more threatening. Those countries with weak surveillance systems may not see early outbreaks until it becomes too late. In politically unstable or humanitarian crisis-affected areas, the virus can spread quietly among unvaccinated groups, only to spill over borders.
Polio flourishes in these crevices—between the unvaccinated, the untracked, and the neglected. And once it establishes itself, retaking control is that much harder and costly.
Although the numbers as they stand are alarming, they also create an opportunity for recommitment on a global scale. Global polio eradication has always been a collective endeavor. Today, more than ever, a concerted effort is needed.
WHO Director-General Dr. Tedros Adhanom Ghebreyesus reacted with strong concern over the diminishing U.S. support and asserted the urgency for international collaboration. "The precipitous cuts to U.S. funding also affect efforts to stop polio for good," he cautioned.
Relaunching public confidence in vaccines, maintaining secure access during times of conflict, reinstating funds channels, and reinforcing surveillance form part of the arsenal necessary to complete the mission against polio.
The resurgence of polio in 2025 is a wake-up call. It reminds the world that public health victories, no matter how close, can unravel quickly without consistent investment and collaboration.
Eradiating polio was never a matter of one country or one continent. It was about a shared global commitment. If the trend continues, we will risk wasting decades of progress—and allowing a preventable disease to reassert its hold on the world's most vulnerable.

Credits: Canva
Why More Women Are Choosing To Have Kids In Their 30s Even As Fertility Drops?
For decades, the ideal age for women to become mothers was firmly rooted in the 20s—a peak period conventionally tied to prime fertility, social norms, and the onset of family life. However, recent information reveals a different picture, more women are increasingly opting to start families when they are in their 30s, although fertility does start decreasing with age. Based on initial data from the Centers for Disease Control and Prevention (CDC), women aged 30 to 34 now have more births than women in their late 20s, a big cultural and demographic change.
This article explores into what's behind this shift—from changing social values and economic considerations to medical innovations and individual empowerment.
In 2016, the CDC also said that the birth rate for women between the ages of 30 and 34 was 103 per 100,000, just barely above the 102 per 100,000 for women between the ages of 25 and 29. The mean age at which American women are giving birth to their first child has also increased to 28, from 26 only a few years earlier. This change signals something more than mere preference; it indicates greater systemic shifts within education, relations, and economic scenarios.
Women aged in their late 20s had the country's peak birth rates for over three decades. That storyline is being revised now. Authorities are attributing the change to a range of interrelated reasons—the primary among them being a decision to wait until marriage to come later in favor of a career or self-realization phase first.
Is Rise of Professional and Financial Independence the Reason?
Women of the millennial and Gen Z generations are entering a job market where education and career mobility are prized—and in many cases, a necessity for financial security. With women becoming more prevalent in positions of leadership within industries and with record-breaking levels of educational attainment, motherhood is no longer viewed as a duty of youth but as a thoughtful life choice.
Waiting until later to have a child offers the time necessary to acquire financial stability, establish a robust professional base, and even eliminate student loans. These actions are important in an environment where living costs and child-rearing—particularly in metropolitan areas—keep increasing.
Deeply connected to this movement is the shifting attitude toward marriage. The first marriage age in America has climbed to 27 for women, a drastic increase over earlier generations. As people delay marriage or pursue alternative relationship structures, the timing of having children has naturally followed suit.
Relationship expert Bill Albert of the National Campaign to Prevent Teen and Unplanned Pregnancy observes that cultural trends, such as the continued decline in teen pregnancies, are part of a larger movement toward thoughtful parenting—where a person is prepared emotionally and economically before assuming the responsibility of bringing a child into the world.
Fertility, Egg Freezing, and Reproductive Health Awareness
Although the social clock might be ticking later, biology hasn't. A healthy woman has approximately a 20% chance of conceiving in any menstrual cycle in her 20s, says the American Congress of Obstetricians and Gynecologists. Fertility, however, starts to decline in the early 30s and declines more steeply after age 37.
Despite this, women are becoming more attuned to these biological facts—and are doing something about it. Egg freezing is becoming a proactive solution, enabling women to freeze their eggs as they work toward other objectives in life. Even though the treatment is expensive (usually more than $10,000, with yearly storage charges), its popularity speaks volumes for the contemporary woman's willingness to seize control of her reproductive destiny.
Infertility Support and Treatment Options
To those who do experience fertility issues, advances in medicine have made family creation more possible than ever. The CDC reports that approximately 11% of women aged 15 to 44 have utilized infertility services, and the Mayo Clinic explains several causes—ranging from ovulation problems and PCOS to endometriosis and cancer treatment complications.
For couples seeking to become pregnant, lifestyle issues such as smoking, weight imbalance, and stress can be factors as well. Health professionals advise women older than 35 to have an evaluation after six months of failing to conceive—six months less than for younger women. With various treatments such as IVF, hormone therapy, and assisted reproductive technologies, increasing numbers of women in their 30s are having successful pregnancies despite the loss of function that comes with age.
Emotional Readiness and the Psychology of Modern Motherhood
Aside from biology and economics, there's the issue of emotional readiness. Women say they feel more grounded, self-assured, and self-aware in their 30s. They've had time to travel, learn, experience the world, and develop a strong sense of self prior to embracing the challenging and life-altering role of motherhood.
This emotional maturity will also feed through into more secure parenting arrangements and more settled family lives. More mature age at motherhood will also include women who have long-term partnership experience and securely structured support networks behind them.
The motherhood narrative is shifting. Women today are rewriting the playbook, using fertility with deliberation and knowledge, and turning conventional wisdom on its head when it comes to the "right" time to have children. While age still plays a huge role in reproductive health, it is no longer the sole factor.
As the world continues to evolve—socially, economically, scientifically, it's bound to happen more and more often that women continue to look on their 30s not as a deadline but as an opening. And as they gain ever-improved access to fertility procedures, as wider society offers their support, as medicine makes breakthrough after breakthrough, they'll have more control over motherhood than ever before to enter into when they want.
Credits: Northwestern Medicine
Breathlessness During Pregnancy? Cough Turned Out To Be Stage 3 Melanoma For This Woman; Doctors Share Details
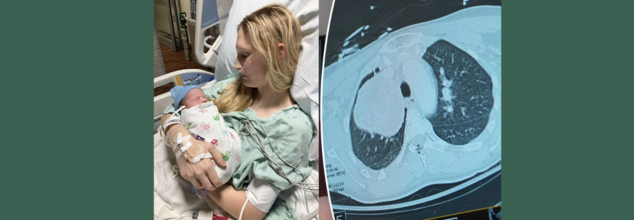
What started out as a persistent cough while pregnant almost turned into a tragedy for 26-year-old Illinois' MaKenna Lauterbach. At 36 weeks' pregnancy, the would-be mom thought that her symptoms were normal for pregnancy exhaustion in late stages—until she started gasping for air from doing minor chores. What ensued was a time-sensitive, life-saving battle of wits between world-class experts, state-of-the-art medical treatments, and an outcome against all odds.
Pregnancy tends to be accompanied by fatigue, shortness of breath, and changing physical needs. So when MaKenna began feeling breathless and having a persistent cough while caring for her horses, she attributed it to third-trimester exertion. Walking to the barn made her breathless—as if she'd run a marathon. But her symptoms did not get better, and by the time she was full term, her condition had progressed dramatically.
Even with her deteriorating symptoms, imaging tests were initially shunned. Medical staff are naturally averse to putting pregnant women through the stress of radiation exposure, particularly when in the late stages of pregnancy. But MaKenna's condition rapidly worsened—coughing gave way to vomiting and intense respiratory distress, prompting emergency admission to hospital.
Just a few days from her due date, imaging at last showed the devastating discovery—a grapefruit-sized tumor wedged in her chest, obstructing the artery to her right lung. The tumor was suffocating her airway and threateningly restricting oxygen delivery, placing mother and baby alike in danger.
MaKenna was flown to Northwestern Memorial Hospital in Chicago, where she was admitted to the intensive care unit. Within a short time after arrival, she went into labor. Her blood pressure rose, the baby became distressed, and physicians realized that they had only hours—possibly minutes—to move.
"Her lungs were impaired because of the tumor, and labor was also slowing her down to breathe. The danger of respiratory failure and cardiac arrest was very real," said Dr. Lynn Yee, a maternal-fetal medicine specialist at Northwestern Medicine.
MaKenna was put on extracorporeal life support (ECMO)—a life-supporting device that circulates oxygenated blood outside of the body—and received an emergency C-section. Her baby boy, Colter, was delivered safely, healthy in spite of the wild ride he had getting here.
For MaKenna, there was a mix of joy and fear. "Because of the tumor, the delivery came so rapidly. I was mourning the birth plan I had been planning for months, while also coping with the news of my surprise diagnosis," she explained.
What is Rare and Aggressive Melanoma?
After the birth, physicians initiated additional tests. A bronchoscopy test showed the tumor was stage 3 melanoma—a skin cancer that had somehow traveled and developed inside her chest.
This posed a singular challenge. "There isn't much written about or a lot of published cases on how to treat melanoma that comes in this way," said Dr. Kalvin Lung, a thoracic surgeon at Northwestern Medicine. "We had to fall back on the knowledge our team has gained from years of taking care of complex thoracic cases."
Prior to surgery, doctors gave three doses of immunotherapy to shrink the tumor. The therapy was effective in diminishing its size from 13 centimeters to 9 centimeters, thus enabling the subsequent action—surgery.
The procedure itself was extremely complicated. Dr. Lung and Dr. Chris Mehta, a cardiac surgeon with Northwestern Medicine, were required to remove MaKenna's right lung entirely, part of the pulmonary artery, and related lymph nodes. The tumor had invaded large blood vessels and spread throughout all three lobes of the right lung. "We may have a case like this every few years," said Dr. Mehta.
Now 27, MaKenna is stable and continues her immunotherapy treatments. Her scans show no new signs of metastatic cancer, and the tumor site remains inactive. She’s focusing on motherhood, recovery, and gratitude.
“Colter is the best baby—always smiling and sleeping through the night,” she said. “I can’t say enough about the incredible medical team that saved my life. Because of them, I’m here today.”
Dr. Yee continued, "To see MaKenna doing so well, and Colter thriving, brings tears to my eyes. It demonstrates what coordinated, compassionate medical care can do."
Can Pregnancy Shadow Life-Threatening Illnesses?
Pregnancy is commonly accompanied by a variety of physical changes—fatigue, shortness of breath, backaches, nausea, and swelling. Although these symptoms are typically harmless, they sometimes mask the signs of serious underlying medical conditions. This crossover between normal pregnancy pains and signs of potentially fatal diseases can mean that the illnesses are not diagnosed until late, as in the recent case of MaKenna Lauterbach—a 26-year-old woman whose relentless cough and shortness of breath throughout her pregnancy proved to be stage 3 melanoma in her chest.
Shared Symptoms of Pregnancy and Illness Mimic One Another
Most life-threatening conditions have symptoms that are identical to those of pregnancy. Diseases such as heart disease, blood clots, infections, and even cancer may appear with fatigue, chest pain, shortness of breath, or swelling—commonly attributed to normal pregnancy complaints. This similarity results in a diagnostic blind spot.
For example:
- Shortness of breath can be due to increased oxygen demand during pregnancy but can also result from lung disease or heart failure.
- Swelling in late pregnancy is normal but may indicate preeclampsia, kidney disease, or a tumor compressing veins.
- Nausea and vomiting are usual in the first trimester but may also obscure gastrointestinal cancers or liver disease.
Hesitation With Diagnostic Imaging in Pregnancy
One of the greatest difficulties is that physicians tend to shun some diagnostic tests such as X-rays, CT scans, or MRIs during pregnancy in order to avoid exposing the fetus to radiation. Although this prudence is necessary, it can lead to life-threatening delays if a critical condition is suspected but not diagnosed. In MaKenna's situation, imaging was delayed until her symptoms became critical—by that time, a tumor had obstructed large lung arteries.
Immune and Hormonal Alterations Can Speed Up Underlying Disorders
Pregnancy dampens some immune reactions to shield the developing fetus. Yet, this changed immune environment can give rise to or speed up latent diseases like cancer, autoimmune disorders, or infections. Hormonal spikes can also nourish hormone-sensitive tumors, elevating the risk of complications.
Fetal Over Maternal Prioritization in Emergency Situations
During emergencies, choices are frequently made to safeguard the baby—even at the expense of delaying the mother's treatment. This preference can make cases more complex when the mother's declining health impacts fetal welfare directly. Delayed diagnosis or treatment of maternal illness can put both lives at increased risk.
Emotional and Cognitive Biases
Numerous pregnant women—such as MaKenna—will minimize their symptoms, assuming they are just a result of pregnancy demands. There is also a cultural pressure to suffer through pregnancy, and this can cause women not to speak up or seek second opinions when something does not feel right.
Pregnant patients with severe medical issues frequently need treatment from several specialists: obstetricians, oncologists, cardiologists, or pulmonologists. Without an integrated and coordinated effort, important warning signs can be overlooked or insufficiently explored. MaKenna's survival was partly because of the rapid collaboration between maternal-fetal medicine, thoracic surgery, oncology, and intensive care specialists.
Pregnancy never needs to stand in the way of diagnosing and treating potentially life-threatening diseases. Awareness, early investigation, and multidisciplinary care are critical in distinguishing normal pregnancy symptoms from red flags. Pregnant women must always feel confident enough to voice their concerns, clarify the situation, and stand up for their well-being—because, as MaKenna's experience demonstrates, an early diagnosis can save not just one, but two lives.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited