- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
'We Have The Means To Prevent 80% Heart Attacks And Strokes', Expert Urges NHS To Give 'Polypill'

Image Credits: Canva
Heart attacks and strokes are among the leading causes of death globally, with millions suffering from cardiovascular diseases (CVD) every year. There are more than seven million people in the UK alone, with about 100,000 patients experiencing heart attacks annually. However, a group of researchers at University College London (UCL) estimate that one 'polypill' taken daily day could eliminate a majority of these cases dramatically lowering death tolls.
The proposed polypill, a combination of a statin and three blood pressure-lowering drugs, has been under study for over two decades. Experts argue that introducing this pill universally for individuals aged 50 and above could be more effective than the current NHS Health Check, which assesses risk factors every five years for those aged between 40 and 74.
Studies have repeatedly proven the effectiveness of the polypill in preventing CVD. A groundbreaking 2019 study in The Lancet found that five years' use of the polypill cut the risk of heart attack and stroke by a third. In addition, previous modelling analyses have estimated that if given universally to people over 55, the polypill might be able to prevent 80% of heart attacks and strokes.
Today, the NHS Health Check follows a risk-based model in which patients are tested for CVD risk factors and treated with drugs accordingly. Yet, as per UCL's study, this system has serious flaws:
Low Uptake: Just 40% of those eligible for the NHS Health Check choose to have it, leaving a considerable number of at-risk patients undiagnosed and untreated.
Ineffective Prediction of Risk: The majority of heart attacks and strokes happen to people at average risk levels, thus making it challenging to identify the need for intervention effectively.
Limited Effectiveness: Even at maximum take-up, the NHS Health Check programme is predicted to have fewer health impacts compared to a polypill initiative applied to the whole population.
Simplicity and Affordability of the Polypill Strategy
One of the big benefits of the polypill is that it is so easy. In contrast to the existing screening-based model, the polypill scheme would not involve complicated medical tests or lengthy risk assessments. Instead, people reaching 50 would just have to fill out a few questions to determine possible side effects before they were prescribed.
Professor Aroon Hingorani of the UCL Institute of Cardiovascular Science, one of the strongest proponents of this scheme, says:
"Finally, the time is now to do much better on prevention. A population approach would prevent a lot more heart attacks and strokes than is done today with a strategy of trying to target a smaller group only."
Aside from the possible health implications, the polypill is also an economic solution. The drugs used are off-patent, thus cheap to produce and distribute. With the vast economic cost of managing CVD-related illnesses, a preventive model could result in substantial cost-saving for the NHS in the future.
The polypill has been proven to be effective by numerous international trials. In 2019, a randomised trial in rural Iran discovered that participants who took the polypill for five years had a 34% reduced risk of having a heart attack or stroke compared to non-participants.
Likewise, modelling research has indicated that even if only 8% of people aged over 50 took up the polypill regimen, it would still be more beneficial to their health than the NHS Health Check programme.
Is This a Case of Over-Medicalisation?
One of the main objections to the polypill strategy is the suggestion that it might result in the unnecessary medicalisation of a significant proportion of the population. But, it is argued, it should be considered as a preventative measure, not as mass medication.
Professor Sir Nicholas Wald of UCL's Institute of Health Informatics explains:
"Instead of being a 'medicalisation' of a significant proportion of the population, a polypill programme is a prevention measure to prevent an individual from becoming a patient."
He compares it with public health measures like water fluoridation or compulsory seatbelts—interventions that have been shown to have a significant impact in reducing public health danger at low individual cost.
With the evidence in favour of the polypill's effectiveness and viability overwhelming, experts are calling on the NHS to act now. It is their belief that substituting the NHS Health Check with a polypill-based prevention program could be the UK government's flagship policy under its pledge to put disease prevention ahead of cure.
As Professor Hingorani points out, "The status quo is not a justifiable option." With CVD still a major cause of death globally, taking a population-wide polypill approach could be a turning point for preventative medicine, potentially saving thousands of lives annually. The question now is whether the NHS will take up this call and establish a policy with the potential to transform the prevention of cardiovascular disease on a national level.
Candida auris Detected in 27 US States: Scientists Reveal How the Deadly Fungus Colonizes Skin
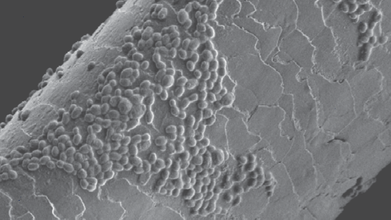
Credit: UCSF
Drug-resistant superbug Candida auris (C. auris) has now been detected in 27 US states. According to the latest data from the US Centers for Disease Control and Prevention (CDC), 3,437 clinical cases have been reported through July 25.
The figure is about 1,000 fewer than the 4,290 cases reported during the same period last year.
Candida auris Remains A Critical Public Health Threat
C. auris is a deadly fungus that primarily poses a concern for people who are hospitalised or in long-term care facilities. The total number of clinical cases has increased since the pathogen was first detected in the US in 2016, the CDC said.
While the rate of increase has slowed in recent years, C. auris remains a “critical public health threat.”
First discovered in Japan in 2009, the pathogen can live silently on the skin but can become deadly when it reaches the bloodstream. It kills about 3,000 patients in US hospitals and long-term care facilities each year.
Now, a new study published in the journal Science has revealed why the deadly superbug can be so difficult to remove from the skin once it takes hold.
How Candida auris Permanently Colonizes Skin
Researchers at the University of California, San Francisco (UCSF) found that C. auris actively rewires the skin’s immune system to protect itself, taking refuge in hair follicles where current therapies cannot reach it.
“Candida auris colonizes skin way better than most other fungi, setting it up to invade once the immune system is weakened,” said Dean Merrill, a dermatologist, UCSF professor and first author of the study.
“The big clinical problem is that we have no effective way to remove it from the skin,” he added.
To understand why C. auris persists on the skin unlike other fungi, researchers compared it with Candida albicans, a common fungus that the skin and immune system normally clear quickly.
In mice, C. auris was found to persist by taking refuge in hair follicles.
While C. albicans activated an immune signal called IL-17, which helps renew the skin’s surface and strengthen antifungal defenses, allowing the infection to be cleared, C. auris, triggered interferon gamma, a signal more commonly associated with viral infections.
The fungus achieved this by remodeling its outer cell wall to expose more of a molecule called chitin. This prompted immune cells to release interferon gamma around the hair follicle.
The interferon gamma then blocked the skin’s antifungal defenses, including IL-17. It also slowed the natural replacement of cells in the hair follicle, causing older, damaged cells to accumulate and creating a niche where C. auris could flourish.
How The Finding Will Help?
The findings reveal potential targets for preventing C. auris from persisting on the skin.
One possible approach could involve drugs that shift the immune response away from interferon gamma and toward IL-17, which drives the skin’s normal antifungal clearing process.
Another possibility could be drugs that block chitin, potentially preventing the fungus from amplifying interferon gamma signals, Merrill said.
More broadly, the researchers say the findings offer a new way of understanding how microbes can quietly coexist with humans before becoming dangerous.
WHO Says Ebola Outbreak Began Months Before It Was Officially Declared; Why Were Early Signs Missed?

Credit: AI
The Democratic Republic of Congo’s (DRC) Ebola outbreak may have been spreading for months before health authorities officially declared it, raising new questions about why the early warning signs were missed.
According to the World Health Organization (WHO), genetic sequencing indicates that the current outbreak began as early as February 2026, while the DRC officially declared the outbreak on May 15. By then, the virus had already had time to spread through communities in eastern DRC.
The outbreak is being caused by the Bundibugyo virus, a rare Ebola species for which there is currently no approved vaccine or specific course of treatment.
What Were The Early Warning Signs?
One of the major reasons why the current Ebola outbreak expanded within a short period of time was that it not immediately recognised.
Some early patients were reportedly treated for malaria or typhoid, illnesses that can initially cause symptoms such as fever, weakness, vomiting and diarrhoea. Early testing also focused on the more common Zaire strain of Ebola, delaying recognition of Bundibugyo virus.
WHO’s own assessment had already identified an unusual cluster of severe illness and deaths in the Mongbwalu health zone in Ituri Province by early May. A subsequent investigation covering April 15 to May 13 identified 246 suspected cases and 65 deaths across three health zones.
Geographical disadvantage was also one of the reasons. Ituri is affected by armed conflict, population displacement and poor road access. Health workers have faced shortages of protective equipment, while some facilities have struggled because of workers' strikes.
Also read: Nova Scotia's Ebola Trial: Why Is Canada Testing A Vaccine When It Has No Outbreak?
What Is The Current Status Of DRC Ebola Outbreak?
The Ebola outbreak in DRC continues to grow at a rapid pace. The latest government figures cited by WHO and international media show about 4,200 confirmed Ebola cases and at least 1,900 deaths in DRC.
WHO Regional Director for Africa Mohamed Janabi described the situation bluntly: “We are chasing the virus, the virus is ahead of us.”
WHO Director-General Tedros Adhanom Ghebreyesus has also warned that the outbreak is moving faster than the response, with cases doubling in some hotspots. He wrote on on X that “the outbreak is spreading faster than our scale up of the response”, adding that new cases had doubled in some hotspots over the previous week.
Ebola becomes considerably harder to contain once transmission moves beyond identifiable limits. Unlike respiratory viruses, Ebola primarily spreads through contact with infected bodily fluids and contaminated materials. But when patients are not recognised early, they can unknowingly expose others, healthcare workers and caregivers.
Also read: FDA Approves Moderna's First mRNA Flu Vaccine, Marking A Milestone In Influenza Prevention
Effects Of Delayed Recognition
One of the major challenges in this outbreak is that around 60–70% of new cases are reportedly occurring outside known contact chains, making traditional contact tracing much harder. The current outbreak has also unfolded in crowded urban and displacement settings, rather than remaining confined to an isolated rural location.
The 2014–2016 West African Ebola epidemic was officially declared in March 2014, although the first human case was later traced back to December 2013. That outbreak eventually led to more than 11,000 deaths.
Progress In Bundibugyo Vaccine Development
The WHO is now pushing to accelerate the response, including clinical trials of the Ervebo vaccine, which is licensed against the Zaire strain but may offer some protection against Bundibugyo. Researchers are also developing vaccines specifically targeting Bundibugyo virus.
mRNA-1469 is an investigational vaccine developed using Moderna's messenger RNA (mRNA) platform, the same technology used in its COVID-19 vaccine. The vaccine builds on the company's broader research into filoviruses, the family of viruses that includes Ebola.
Experimental Menopause Drug Shows Promise Mid-Stage Trial, Reduces Hot Flashes By 83%

Credit: AI
A new experimental menopause drug has shown promising results in reducing hot flashes, with the company reporting an 83% reduction in moderate-to-severe episodes in a mid-stage clinical trial.
Shares of Canadian biotechnology company AbCellera surged nearly 40% on Monday after it announced positive results for ABCL635, an experimental non-hormonal treatment for moderate-to-severe vasomotor symptoms associated with menopause.
The Phase 2 study involved 92 women. After four weeks, women who received a single 600-mg dose of ABCL635 experienced an 83% reduction in the frequency of moderate-to-severe hot flashes, equivalent to 8.8 fewer episodes per day from baseline. The placebo group reported a 33% reduction, or 3.5 fewer episodes per day.
The treatment also improved the severity of symptoms, sleep and women's overall assessment of their improvement, according to the company.
The most commonly reported side effects, however, included headache, fatigue and reactions at the injection site.
What Makes This Drug Significant?
ABCL635 takes a different approach from hormone replacement therapy (HRT). It is a non-hormonal antibody treatment that targets the neurokinin 3 receptor, or NK3R, a protein involved in the brain's regulation of body temperature.
During menopause, falling estrogen levels can disrupt the activity of a group of brain cells known as KNDy neurons. This can make the body's temperature-control system overly sensitive, triggering hot flashes. By blocking NK3R signaling, ABCL635 is designed to help restore that balance.
Also read: Lifestyle Genetics And Hormones: Understanding The Interplay Of Risk Factors For Ovarian Cancer
More About The Drug
One of the drug's potential advantages is its dosing. ABCL635 is being developed as a long-acting, once-monthly injection, rather than a daily pill.
AbCellera's chief medical officer Sarah Noonberg said the approach could appeal to women already accustomed to self-injecting medicines and could potentially improve adherence compared to daily dosing.
When the Phase 2 programme began, Noonberg said: “Menopausal symptoms can have a profound impact on quality of life,” adding that the company wanted to assess whether ABCL635 could offer women a safe and effective non-hormonal alternative.
However, the drug is still experimental and has not been approved for clinical use. AbCellera said additional 12-week trial data are expected later this year, which will provide a better picture of how long the benefits last and how the treatment performs over a longer period.
The drug development comes as non-hormonal menopause treatments are gaining popularity. FDA-approved options already include drugs targeting neurokinin pathways, including Astellas' Veozah and Bayer's Lynkuet, giving women alternatives when hormone therapy is unsuitable or not preferred.
Why Menopausal Hot Flashes Can Be Unnerving?
Hot flashes, also known as vasomotor symptoms, are among the most common symptoms of menopause. The Menopause Society says up to 80% of women experience hot flashes or night sweats at some point during the menopause.
A hot flash can begin suddenly, often as an intense wave of heat across the face, neck and chest. It may be followed by sweating, chills, dizziness, anxiety or racing heartbeat. When these episodes happen during sleep, they are known as night sweats.
Frequent hot flashes can repeatedly interrupt sleep, leaving women irritable and fatigued the next day. Poor sleep can then affect concentration, mood and daily functioning, creating a cycle in which one menopause symptom amplifies another.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited