- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
Japan Could Become The First Country To Eradicate HIV
Credits: Canva
Japan could become one of the first countries in the world to end the HIV epidemic, says the president of Gilead Sciences Japan, Kennet Brysting. The idea for now could seem a little too ambitious, but it is not entirely unrealistic, given that the availability of medicines that can prevent transmission of HIV. Drugs are not the cure, but control over the spread of virus to the point where the disease is no longer a major public health threat.
What Is The Role Of Preventative HIV Medicines?
Gilead's have two key drugs, Truvada and lenacapavir. These two are playing a crucial role in prevention. Truvada is taken as a daily pill, while lenacapavir requires two injections per year. It can make the virus undetectable in infected individuals and prevent transmission to those who are not infected yet. In trials, lenacapavir showed 100% efficacy in preventing HIV infections. This is why it is describe as "almost a vaccine".
In 2024, Japan also approved Truvada for HIV prevention, but the country has yet to approve lenacapavir for the same. Until now, people in Japan had been importing generic versions of Truvada or purchasing it from clinics that source it from overseas.
HIV In Japan
Up until now, Japan reported around 25,000 HIV infections, whereas 669 new cases were reported in 2023. For seven consecutive years, the number of new infections remained under 1,000. The downward trend thus shows that the virus has been controlled, however, getting to zero new infections remains the ultimate goal.
Brysting too acknowledged that simply having effective drug is not enough. What is important is to have a proper implementation, access and healthcare support to make sure that these treatments are widely available and effective.
What Are The Challenges In Implementation?
The biggest challenges is testing rates. There is a need to increase testing rates. At this very moment, around 86% people infective with Japan have been tested, but the goal is to increase it up to 95%, with an ideal goal of 100%. Without widespread testing, many infected people may not even know that they are infected and it could transmit the virus.
Another measure issue is the cost of preventative medication. While Japan's health insurance covers treatments for diseases, it does not cover preventative drugs. Those who purchase Truvada for prevention, pay around $470 per month. Some clinics in Tokyo offer generic alternatives too, which is cheaper, but they are not ideal.
Better Healthcare Support
Brysting expressed concern that individuals importing medications might not be consulting doctors regularly, which is essential for monitoring HIV status and overall health. Truvada users need to be tested for HIV initially and every three months, along with screenings for other infections and kidney function checks. Without proper medical supervision, there is a risk of misuse and inadequate protection.
Gilead is in discussions with Japanese authorities to improve access and insurance coverage for Truvada, and progress is being made. Japan has shown efficiency in approving critical medicines, as seen during the COVID-19 pandemic when Gilead’s remdesivir was approved in just three days.
What Is The Way Ahead?
Gilead at this moment is not only focused on HIV and hepatitis C, but also expanding into oncology with innovative treatments like CAR-T cell therapy, which strengthens a patient's immune system to fight cancer.
However, Japan’s strict approval processes can slow down drug availability. Phase 3 clinical trials often need to be conducted within the country, and Japan tends to approve medicines much later than other regions. For instance, Truvada was approved for prevention in Japan 12 years after the U.S. and nearly 20 years after its approval for treatment. inancial factors also play a role. The Japanese government adjusts drug prices annually, often reducing them, which can make long-term investment challenging for pharmaceutical companies.
Kennedy Announces Food Policy Reforms Under Trump’s MAHA Agenda: What Has Been Proposed?
Credit: AP Photo
US Department of Health and Human Services (HHS) Secretary Robert F. Kennedy Jr. has announced food policy reforms as part of efforts to implement President Donald Trump’s Make America Healthy Again (MAHA) initiative.
The proposed measures focus on two areas: greater oversight of food ingredients and establishing a standardized federal definition of ultra-processed foods.
As per Kennedy, “nearly 60% of the American diet is made up of ultra-processed foods, and childhood obesity now affects more than one in five American children”.
To counter this, transforming the food system is key, he said.
“These historic actions bring greater transparency to what’s in our food and stronger science to federal nutrition policy. President Trump and I promised to Make America Healthy Again, and today we are turning that promise into policy,” Kennedy said.
What Are the Proposed Changes?
HHS has proposed a rule that would require manufacturers to notify the US Food and Drug Administration (FDA) when they determine that a substance added to human or animal food is Generally Recognized as Safe (GRAS).
In addition, HHS and the US Department of Agriculture (USDA) have submitted for final review the federal government’s first proposed definition of ultra-processed foods (UPFs).
Acting FDA Commissioner Kyle Diamantas said the measures are intended to increase transparency and strengthen science-based oversight of ingredients entering the food supply.
“By proposing mandatory GRAS notifications, we are closing critical information gaps and giving the FDA greater visibility into substances entering the food supply,” Diamantas said.
He added that the proposed UPF definition could provide a stronger foundation for future nutrition research.
What Is GRAS?
GRAS stands for Generally Recognized as Safe. It refers to substances that are considered safe by qualified experts for their intended use and are therefore exempt from the standard premarket approval requirements for food additives.
Examples of GRAS ingredients include canola oil, vinegar and spices such as black pepper.
Under the proposed rule, manufacturers would be required to notify the FDA when they conclude that a substance qualifies as GRAS. The agency would also expand its public-facing inventory of submitted GRAS notices.
According to Diamantas, mandatory notifications would help close information gaps and give the FDA greater visibility into substances entering the food supply.
First Federal Definition of Ultra-Processed Foods
HHS and USDA have submitted for final review the federal government’s first proposed definition of ultra-processed foods.
Research has linked high consumption of UPFs with preventable chronic diseases, including type 2 diabetes and heart disease. However, the absence of a standardized federal definition has made it difficult to maintain consistency in research across federal agencies.
The proposed definition incorporates feedback from thousands of stakeholders, including industry representatives, consumer organizations, researchers and members of the public.
Diamantas said the definition could help “create a stronger foundation for future nutrition research.”
How Does This Support Trump’s MAHA Agenda?
The measures are part of the Trump administration’s Make America Healthy Again Strategy and build on efforts to strengthen nutrition science, improve transparency and modernize oversight of the US food supply.
HHS also encouraged Congress to build on these efforts through legislation aimed at further strengthening the safety of the American food supply.
Ebola Death Toll Tops 2,000 In DRC: New Study Reveals Likely Source Of Bundibugyo Virus Outbreak
Credit: iStock
The death toll from Ebola has crossed 2,000 in the Democratic Republic of the Congo (DRC), three months after the outbreak was officially declared in May.
The outbreak has caused 4,381 confirmed cases across five provinces, making it the fastest-growing Ebola outbreak recorded in the Central African country. The response has been complicated by strikes by unpaid health workers, misinformation and cultural practices.
Ebola Virus Outbreak Began in February
The outbreak is caused by the rare Bundibugyo strain of Ebola, for which there is currently no approved treatment or vaccine.
According to the World Health Organization (WHO), the virus first emerged in the DRC in February, about three months before the outbreak was officially declared in the DRC and neighboring Uganda on May 15.
Some early patients were reportedly treated for malaria or typhoid, which can initially cause fever, weakness, vomiting and diarrhea. Early testing also focused on the more common Zaire strain of Ebola, delaying recognition of the Bundibugyo virus.
By early May, WHO had identified an unusual cluster of severe illness and deaths in the Mongbwalu health zone in Ituri Province. An investigation covering April 15 to May 13 subsequently identified 246 suspected cases and 65 deaths across three health zones.
The response has also been affected by conditions in Ituri, including armed conflict, population displacement and poor road access. Health workers have faced shortages of protective equipment, while some healthcare facilities have been affected by workers' strikes.
Zoonotic Spillover Likely Triggered the Outbreak
A new study published in Nature Medicine suggests that the outbreak began through a zoonotic spillover event, meaning the virus jumped from animals to humans before spreading between people.
Researchers from Congo, Uganda, Belgium and other countries found that the outbreak strain was genetically distinct from Bundibugyo Ebola viruses identified during previous outbreaks in 2007 and 2012.
The findings are consistent with a new animal-to-human transmission event, followed by sustained human-to-human transmission.
The study did not identify the specific animal source. However, Ebola viruses are known to periodically spill over from infected animals into human populations.
Genetic analysis also confirmed that cases detected in Uganda were linked to the outbreak in Congo.
How Was the Study Conducted?
Bundibugyo virus disease (BVD) outbreaks were previously recorded in 2007–2008 in Bundibugyo District, Uganda, and in 2012 in Isiro, DRC.
For the 2026 outbreak, researchers generated 22 viral genomes from samples collected from patients with BVD in the DRC and Uganda.
The genomes formed a well-supported phylogenetic cluster separate from variants associated with the 2007 and 2012 outbreaks. The analysis also showed evidence of sustained human-to-human transmission.
The researchers called for greater decentralized laboratory diagnostic capacity, including pan-Orthoebolavirus testing and genomic sequencing, to improve early detection and control of future outbreaks.
How Does Ebola Spread From Animals to Humans?
Ebola can jump to humans from infected animals such as bats, monkeys and apes. Transmission can occur through contact with blood, body fluids, excrement or raw meat during hunting and butchering.
Once the virus enters the human population, it can spread from person to person through contact with infected bodily fluids.
Symptoms of Bundibugyo Virus Disease
Symptoms of Bundibugyo virus disease are similar to those caused by other Ebola viruses and can include:
- Fever
- Headache
- Muscle pain
- Weakness
- Diarrhea
- Vomiting
- Stomach pain
- Unexplained bleeding or bruising, usually in later stages of illness
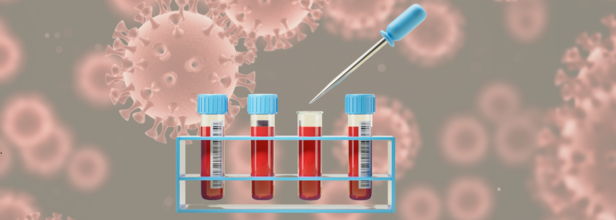
One Blood Test For Multiple Cancers? New Study Shows Promise In Early Detection

Credit: AI
What if one blood sample could detect symptoms of multiple cancers at once, while also disclosing which organ may be affected? A new study from UCLA has brought that possibility a step closer to reality.
Researchers have at UCLA have developed a blood test called MethylScan that can detect molecular signals linked to multiple cancers and other diseases by analysing DNA fragments circulating in the bloodstream.
The findings, published in the Proceedings of the National Academy of Sciences, suggest the test could offer a simpler and potentially cheaper way to screen for serious diseases like cancer before their symptoms appear.
How Can One Blood Test Detect Different Cancers?
A blood test may be able to detect multiple cancers at once due to cell-free DNA (cfDNA). Every day, billions of cells die and release tiny fragments of DNA into the bloodstream. These fragments carry information about where they came from and what is happening in that tissue.
Instead of primarily searching for cancer-causing mutations, MethylScan looks at DNA methylation, a type of chemical tags that regulate how genes behave.
Different organs have distinct methylation patterns, and those patterns can change when cells become cancerous or diseased.
“DNA methylation reflects the health status of a tissue. It’s a very informative signal,” said Dr Wenyuan Li, professor of pathology and laboratory medicine at UCLA.
The researchers also developed a method to filter out the DNA released by normal blood cells, reducing the "background noise” that can make early cancer signals difficult to detect.
What Are The Study's Findings?
The researchers tested MethylScan using blood samples from 1,061 people, including patients with liver, lung, ovarian and stomach cancers, people with liver diseases and healthy participants.
At 98% specificity, the test detected about 63% of cancers across all stages. For early-stage cancers, its sensitivity was around 55%.
The test also showed promise in identifying where an abnormal signal originated. This could help as a positive blood test would still need to be followed by imaging or other diagnostic tests.
“Being able to trace signals back to their source is important because a positive blood test needs to be followed by imaging or other diagnostic procedures directed at the right organ,” Li said.
Also read: Tudriqev: US FDA Approves Replimune's Skin Cancer Drug After Rejecting It Twice
Early Cancer Detection Is Key
“Early detection is crucial,” said Dr Jasmine Zhou, the study’s senior author. “Survival rates are far higher when cancers are caught before they spread.”
The findings are promising, but larger trials will be needed to establish whether such tests can reliably detect cancers in people who have no symptoms.
Also read: Following A Western Diet? Changes In Your Gut Bacteria Could Increase Colon Cancer Risk
More Developments In The Field
The findings come as another multi-cancer test, Galleri, is designed to detect signals from more than 50 cancers from a single blood sample.
Reuters reported this month that the US FDA plans to convene an advisory panel in September to review its application for approval.
But experts continue to stress that these tests are not replacements for established screening, such as mammograms or colonoscopies.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited